
Page 122 - Buku Panduan Perkhidmatan MKAKB
P. 122
MKAK-BPU-U01
Lab No. (for lab use) :
REQUESTOR INFORMATION
Name :
Post : MAKMAL KESIHATAN AWAM KEBANGSAAN
Address : KEMENTERIAN KESIHATAN MALAYSIA
District : State : Lot 1853, Kg Melayu Sungai Buloh,
Tel. No. : Fax No. : 47000 Sungai Buloh, Selangor Darul Ehsan
Email : Tel: 03-61565109 Fax: 03-61402249/61569654
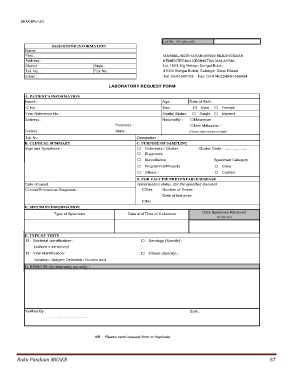
LABORATORY REQUEST FORM
A. PATIENT'S INFORMATION
Name : Age : Date of Birth :
IC No : Sex : Male Female
Your Reference No. : Marital Status: Single Married
Address : Nationality : Malaysian
Postcode : Non Malaysian :
District : State : (Please state country of origin)
Tel. No : Occupation :
B. CLINICAL SUMMARY C. PURPOSE OF SAMPLING
Sign and Symptoms : Outbreaks / Cluster Cluster Code: ……………….
Diagnostic
Surveillance Specimen Category :
Programme/Projects Case
Others : Contact
D. FOR VACCINE PREVENTABLE DISEASE
Date of onset : Immunisation status (for the specified disease)
Clinical/Provisional Diagnosis : Yes Number of Doses :
Date of last dose :
No
E. SPECIMEN INFORMATION
Type of Specimen Date and Time of Collection Date Specimen Received
(for lab use)
F. TYPE OF TESTS
Bacterial identification : Serology (Specify) :
(culture ± sensitivity)
Viral Identification : Others (Specify) :
Isolation / Antigen Detection / Nucleic acid
G. RESULTS (for laboratory use only) :
Verified By : Date :
………………………..
NB : Please send request form in duplicate
Buku Panduan MKAKB 87