
Page 123 - Buku Panduan Perkhidmatan MKAKB
P. 123
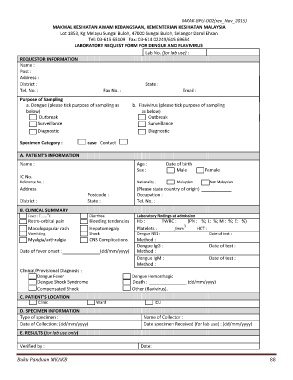
MKAK-BPU-D02(rev_Nov_2015)
MAKMAL KESIHATAN AWAM KEBANGSAAN, KEMENTERIAN KESIHATAN MALAYSIA
Lot 1853, Kg Melayu Sungai Buloh, 47000 Sungai Buloh, Selangor Darul Ehsan
Tel: 03-615 65109 Fax: 03-614 02249/615 69654
LABORATORY REQUEST FORM FOR DENGUE AND FLAVIVIRUS
Lab No. (for lab use) :
REQUESTOR INFORMATION
Name :
Post :
Address :
District : State :
Tel. No. : Fax No. : Email :
Purpose of Sampling
a. Dengue (please tick purpose of sampling as b. Flavivirus (please tick purpose of sampling
below) as below)
Outbreak Outbreak
Surveillance Surveillance
Diagnostic Diagnostic
Specimen Category : case Contact
A. PATIENT’S INFORMATION
Name : Age : Date of birth
Sex : Male Female
IC No.
Reference No. : Nationality : Malaysian Non Malaysian
Address (Please state country of origin) ____________
Postcode : Occupation :
District : State : Tel. No. :
B. CLINICAL SUMMARY
o
Fever : T ……. C Diarrhea Laboratory findings at admission
Retro-orbital pain Bleeding tendencies Hb : TWBC : (PN : %; L: %; M : %; E: %)
3
Maculopapular rash Hepatomegaly Platelets : /mm HCT :
Vomitting Shock Dengue NS1 : Date of test :
Myalgia/arthralgia CNS Complications Method :
Dengue IgG : Date of test :
Date of fever onset : (dd/mm/yyyy) Method :
Dengue IgM : Date of test :
Method :
Clinical/Provisional Diagnosis :
Dengue Fever Dengue Hemorrhagic
Dengue Shock Syndrome Death : (dd/mm/yyyy)
Compensated Shock Other (flavivirus).
C. PATIENT’S LOCATION
Clinic Ward ICU
D. SPECIMEN INFORMATION
Type of specimen : Name of Collector :
Date of Collection: (dd/mm/yyyy) Date specimen Received (for lab use) : (dd/mm/yyyy)
E. RESULTS (for lab use only)
Verified by : Date:
Buku Panduan MKAKB 88